
From trauma to healing
How tools developed by UWM researchers are helping families and communities
Enilda Burgos is a caseworker at UMOS, a social services agency tucked into a south side Milwaukee neighborhood. She assists and supports chronically unemployed adults as they attend mandatory employment counseling sessions, which are designed to help them find steady work.
Life complicates employment prospects for these adults, each a parent receiving government assistance. Many have experienced significant trauma that’s had lasting effects, and Burgos gets only a brief glimpse into their lives outside her cubicle walls. This can make it hard to provide the important help people need, as was the case with one longtime client who struggled to attend her monthly UMOS appointments.
Trust is a barrier for people who have survived complex trauma. Time is a barrier for caseworkers who have 30 or more clients. Tools like T-SBIRT can help overcome both obstacles simultaneously.
Burgos knew the woman had a history of anxiety, but she didn’t feel comfortable asking many questions about it during their brief and sporadic meetings. Then Burgos and her team met Dimitri Topitzes, an associate professor of social work in UWM’s Helen Bader School of Social Welfare. A former licensed clinical social worker himself, Topitzes trained UMOS caseworkers to better assess the mental health needs of their clients and helped streamline referrals for those needing more urgent psychological support.
Topitzes and Josh Mersky, a Helen Bader School professor of social work, are experts in building relationships and working with social welfare agencies to implement practices that better serve clients. They’re co-founders of the Institute for Child and Family Well-Being, a collaboration with Children’s Hospital of Wisconsin that has the mission of improving the lives of children and families.
Topitzes and Mersky want their work and research to have an impact on individuals and the broader policies and systems that exist to help them. “So that vulnerable families have access to the best experiences and services available to them,” Topitzes says, “based on the science.”
Part of their research involves creating tools, such as screening surveys, and embedding them at UMOS and more than a dozen other Wisconsin health and social service agencies to assess and improve their effectiveness. One such tool is a screening protocol called T-SBIRT, short for Trauma Screening, Brief Intervention, Referral to Treatment. For folks on the receiving end, it feels like a guided conversation that introduces the concept of trauma, seeks permission to ask about their personal history of trauma and then asks how they deal with stressful life events.
Eventually, Burgos’ client met with Topitzes, who helped Burgos administer T-SBIRT. In a 15-minute motivational interview, T-SBIRT can nudge people closer to healing by acknowledging their innate coping skills. It also enhances trust with a caseworker or mental health professional, who then makes referrals for long-term mental health care.
“It wasn’t until we administered T-SBIRT that I knew this woman had suffered beatings and sexual assault,” Burgos says. “Until that moment, we weren’t able to connect all the pieces and understand why these things – absences and anxiety – kept happening to her.”
Trust is a barrier for people who have survived complex trauma. Time is a barrier for caseworkers who have 30 or more clients. Tools like T-SBIRT can help overcome both obstacles simultaneously. “For our clients,” says Lisa Ortiz, who oversees Burgos and four other caseworkers, “it changes their focus from ‘What’s wrong with me?’ to ‘Here’s what’s happened to me, and how can I heal from this?’”


A Duo in Dialogue
Trauma can take many forms, and it can stem from sudden events or accumulate over many years. Sometimes, poverty creates trauma. A childhood lived in poverty – wondering where the next meal comes from – can interrupt a child’s growth and development.
Other times, poverty is a symptom of trauma. Left untreated, traumatic episodes accumulate like a pile of bricks. Researchers call this complex trauma. It can make things in life much more difficult, from raising a child to finding a job.
Moving conversation to the forefront of publicly funded, trauma-responsive practices is a hill Mersky and Topitzes have been climbing for years. They met in 2001 at UW-Madison, and both earned their doctorates in social work there. About a decade ago, their paths merged again at UWM, where their shared research interests led to establishing the Institute for Child and Family Well-Being in 2016. The institute focuses on designing and implementing effective programs, conducting cutting-edge research and program evaluations, and promoting change through policy and advocacy.
Mersky and Topitzes work largely as a team. They provide training to health and human services personnel, and they interact with the clients of partner agencies, as Topitzes did in administering the T-SBIRT. They also handle administrative duties. This includes having meetings and phone calls with research partners, recruiting new partners, and collecting data from agencies using T-SBIRT and other survey tools.
Their partnerships and working relationships with organizations such as UMOS, the Central Racine County Health Department and others is a testament to how far their work has come.
“When we first started down this road,” Mersky says, “I can tell you that many practitioners we interacted with –”
“Most of them,” Topitzes quietly interjects.
“Were squeamish,” Mersky continues, “about asking their clients these kinds of questions. The concern is always: ‘What happens if I ask?’ But you have to be able to counter that with: ‘OK, what happens if I don’t ask?’ Is the trauma not there? Have they not had these experiences?”
For Topitzes and Mersky, the answer has long been clear. Even before Topitzes developed the T-SBIRT protocol, he and Mersky adapted other trauma-screening surveys and completed evaluations of trauma exposure at the individual and community level. Doing so offered a wide-angle view that was missing from older screening tools, which were largely based on the experiences and needs of more affluent, less diverse populations.
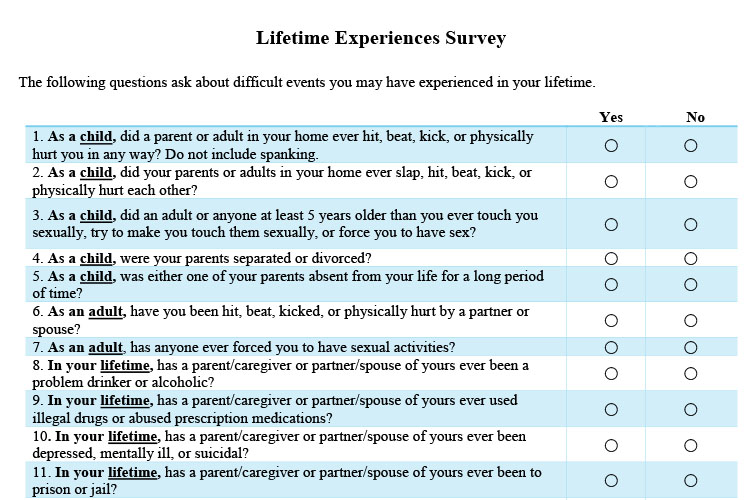
The results were three new screening tools: a Childhood Experiences Survey, an Adult Experiences Survey, and a Lifetime Experiences Survey that measures exposure to childhood and adult trauma. The surveys were designed to promote respectful conversations rooted in trust and consent, an approach that serves as the foundation for their work.
These tools addressed the challenges of growing up in less-affluent urban communities, including generations of unemployment, gun violence, and a lack of affordable health and mental health care. “Bad things don’t just happen to you in your household. They can happen in your community,” Mersky explains. “Our surveys ask nine new questions about poverty, homelessness, exposure to neighborhood violence, exposure to bullying or peer victimization.”
The surveys are used to assess people’s experiences with complex trauma in order to better address its aftereffects. Portions were later incorporated into T-SBIRT.
“One thing that you can do about trauma,” Mersky says, “is ask people questions about it.”
Meeting the Challenges
In cities like Milwaukee and Racine, officials have realized they can’t afford to not ask difficult questions about poverty, neighborhood violence and sexual abuse.
No single approach or initiative can address these social issues entirely. But Mersky and Topitzes believe their work can help. “Milwaukee does have significant challenges,” Mersky says, “but that’s part of what motivates us to do work here.”
It also motivates them to take a long-term view when implementing their work. “We’re not just interested in developing a one-off intervention and testing it in a clinical controlled setting in a university and then publishing our findings,” Mersky says.
“We’re funded by county and state government,” Topitzes adds. “Hence, the programs, practices, interventions we’re investigating are ones our funders are interested in sustaining over the long haul.”
One example is the Family Connects pilot home-visiting program, a partnership between the institute and the Central Racine County Health Department.
Since July 2017, every woman who delivers a baby at Ascension All Saints Hospital in Racine has been asked the same question one day after her baby’s birth, and always by a nurse: “Would you like a follow-up home visit from one of our staff nurses?” About 75 percent of new moms say yes. By three weeks postpartum, about two-thirds of them have completed their home visit through Family Connects.
The program attempts to reach families, determine who needs the most support and then refer mothers to resources they need, such as a crib, job training, mental health care or housing referrals, all aligned by public health nurses.
Before the program’s implementation, Topitzes traveled to Durham, North Carolina, with Jeffrey Langlieb, Central Racine County Health Department’s community health director, to study the original Family Connects program as a model. Durham’s Family Connects has led to significantly fewer child abuse cases in its coverage area, and it follows the standard home-visit pattern, with a twist. Instead of visiting only moms who live at or below the federal poverty line, it reaches out to all moms, regardless of income.
“If you want to move a needle like child maltreatment,” Topitzes explains, “this requires us to reach as much of the population as possible.”
Topitzes and Langlieb interviewed the Durham program’s founders and participated in recruitment activities. Research continued in Racine. “Instead of coming in and telling our nurses what to do,” Langlieb explains, “Dimitri went through three or four meetings to really learn about how our nurses do their work.”
Racine home visits include an interview protocol that Topitzes and Mersky have developed. It incorporates questions from T-SBIRT and the Lifetime Experiences Survey. Topitzes says the approach is effective and subtle: Ask about a mom’s positive stress-management techniques, seek permission to ask about harmful coping strategies, then offer any necessary referrals to treatment.
He describes it as building trust and softening resistance to referrals. Family Connects is embedded within Racine’s network of social service and medical providers, so whether a mom needs child care, a car seat or a new family doctor, the visiting public health nurse can make the right referrals.
If Family Connects works in Racine – and data shows about 50 percent of new moms act on their referrals – Mersky and Topitzes plan to scale up the program in Milwaukee. Their goal is to see universal family home-visiting become the standard of care statewide. They hope it will be one more way to help people move down the path from trauma to healing.
“Resilience is not special to one person over another,” Mersky says. “We all have the capacity to recover or heal.”