The mission of the Institute for Child and Family Well-Being is to improve the lives of children and families with complex challenges by implementing effective programs, conducting cutting-edge research, engaging communities, and promoting systems change.
The Institute for Child and Family Well-Being is a collaboration between Children’s Wisconsin and the Helen Bader School of Social Welfare at the University of Wisconsin-Milwaukee. The shared values and strengths of this academic-community partnership are reflected in the Institute’s three core service areas: Program Design and Implementation, Research and Evaluation, and Community Engagement and Systems Change.
In This Issue
- Meet the ICFW – Zoom and 4th Anniversary Edition
- Community Engagement & Systems Change
- Research and Evaluation
- Program Design & Implementation
- Recent and Upcoming Events
Meet the ICFW
As both Children’s Wisconsin and the University of Wisconsin-Milwaukee implemented “safer-at-home” policies in mid-March in alignment with the best practice and safety guidelines provided to protect our health, “flatten the curve”, and support our essential workers and frontline healthcare providers during these times of COVID-19, we have leaned heavily on Zoom and other technologies to continue to do our work and meet as a team.
The Institute for Child and Family Well-being recently celebrated its 4th anniversary during this first week of May! We will be celebrating with one another from a safe distance via Zoom and phone calls.
Children’s Wisconsin’s ICFW Team (not pictured: Jenni Scott)

ICFW Leadership Team (not pictured: Jenni Scott)

Community Engagement & Systems Change
The Institute develops community-university partnerships to promote systems change that increases the accessibility of evidence-based and evidence-informed practices.
Non-profit and Systems Innovation in Times of COVID-19
At the Institute for Child and Family Well-being, our mission is to improve child and family well-being through the design and implementation of effective practices that reflect the best and latest research, so that we may promote systems change that engages and serves our community. We recognize that COVID-19 poses challenges today that require innovative practices and policies that draw on established evidence to provide the best possible care to our community, and opportunities to learn from those practices and policies that may lead to more resilient and supportive communities in the future.
In order to effectively meet this challenge, we must first acknowledge that the need to maintain physical distance (or “social distancing”) and wearing masks have the potential to have more adverse impacts on our most vulnerable and historically oppressed families and communities. Within the communities where our most vulnerable families live, our systems are often disjointed or insufficient to meet their challenges around access to quality health care, job and housing insecurity, and under-resourced schools, particularly in times like this. These same children and families are also more likely living in high concentration neighborhoods with multiple generations or families in the same home and higher concentration of apartment complexes, which increases risk of infection. In the absence of responsive social connections, these challenges can create high levels of toxic stress and, consequently, greater likelihood of substance abuse, untreated mental health symptoms, violence, and involvement with the child welfare and criminal justice systems.
Since the beginning of the COVID crisis, our ICFW Children’s Wisconsin team has asked “How might we develop innovative practices to meet these challenges today?” The following is our current set of answers and commitment to our community:
- We developed and will facilitate a Community of Practice across our Children’s Wisconsin Community Services and Community Health programs that will promote shared strategic learning and planning around the following:
- Innovative practices that address COVID-19 challenges through family and community engagement, collaboration, program adaptation, etc;
- Positive stories about how a COVID-19 challenge was met, and children and families benefitted;
- Tips for working remotely to improve how we meet these demands under new and challenging working conditions.
- Highlight community efforts and positive stories; and share supportive resources to enhance access to social connections and basic needs, and the latest research and science to reduce the likelihood of infection.
- We will work closely with our community, academic and health partners to seek innovative and compassionate solutions to these complex challenges through human-centered design, prototyping and strategic learning, so that children and families may remain healthy while also remaining connected to those that they need and trust for their well-being.
More recently, our team began asking “How might we learn from the conditions that led to today’s challenges and how we respond to imagine more resilient, supportive and prosperous communities and systems in the future?” When we consider the role that social determinants of health play in one’s ability to overcome the challenges created by COVID-19, we must propose and develop transcendent solutions much like the Beveridge report did at the height of the Second World War. Formally known as the Social Insurance and Allied Services, the report noted the social and economic devastation that was looming in post-war Britain if a social safety net and national healthcare system weren’t created. The Report, which drew on surveys of British citizens, existing evidence, and policy proposals that were previously considered politically impossible, would serve as the blueprint for Britain’s National Health Service, Maternity and Pension Plan, and major labor and housing reforms. As you will see in some of our articles throughout this newsletter, we have tremendous challenges and, therefore, great potential for change within our child welfare, mental and behavioral health, and housing systems, to name just a few. So, let’s ask ourselves, “How might we understand this unprecedented challenge from a community and systems perspective, so that we may propose and develop solutions that build more resilient, healthy and prosperous communities for all?”
Learn More:
The Next Challenge of the COVID-19 Fight in Milwaukee – Reggie Jackson
The Beveridge Report and its Impacts on British Policy and Society
Rethinking Social Change in the Face of Coronavirus – Stanford Social Innovation Review
Child Welfare in Times of COVID-19
By Colleen Janczewski, Gabriel McGaughey, and Josh Mersky
We are in unprecedented times. COVID-19 is ravaging our health and economic infrastructure, with untold losses still to come. Globally and nationally the pain of the pandemic is widespread, and it is a particularly dire situation for those among us who are most vulnerable. These include individuals and families who struggle with extreme poverty, housing insecurity, substance use, health and mental health problems, and chronic stress. Even in good times, these challenges are difficult to bear. But now they are compounded by social distancing from the connections that protect us in times of stress—our families, friends, schools, places of worship, and communities.
These tragic conditions will have a profound impact on children, especially those who need protection. At a point when they are most developmentally sensitive, many are being exposed to adverse experiences that will have lasting neurobiological, cognitive, social and emotional consequences. It is a stark reality that, as our lives are being upended, some children are being abused and neglected. Worse still, these children are being dislocated from the social institutions and connections that are in place to protect them.
To illustrate the magnitude of the problem, consider that child protective service (CPS) agencies in the U.S. received over 4.3 million abuse and neglect reports in 2018, representing approximately 7.8 million children. Although most reports are not investigated or substantiated, CPS records indicate that hundreds of thousands of children are abused or neglected each year. Of course, many more children experience trauma that goes unseen or unheard.
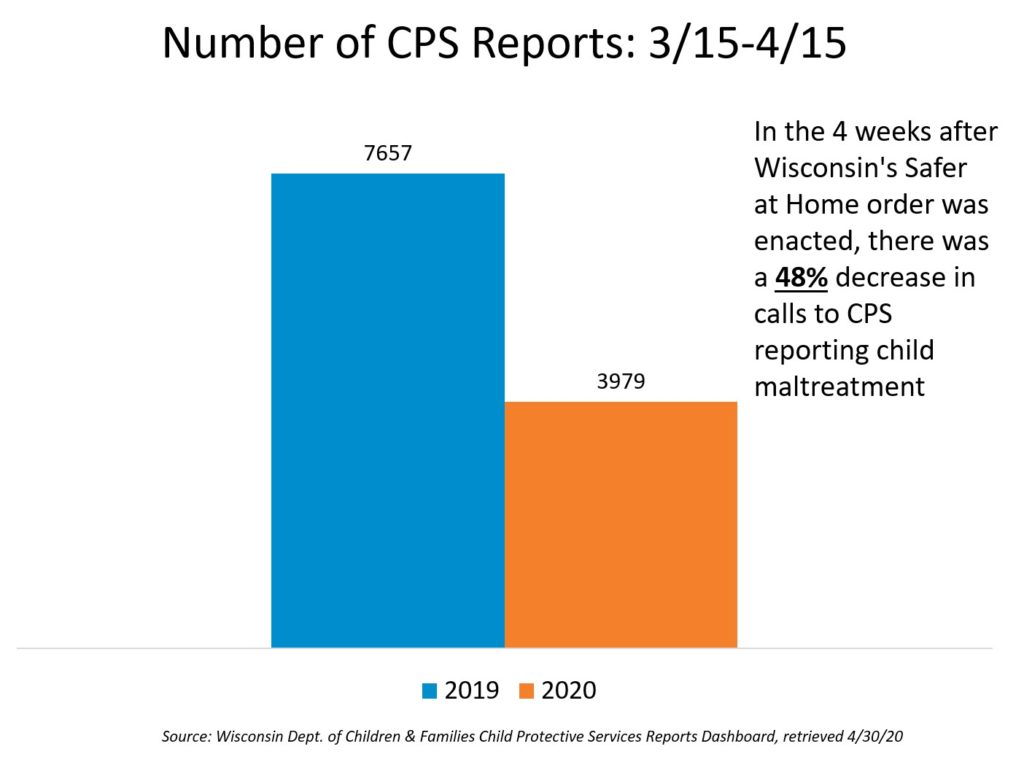
Now consider that, at a time when our most vulnerable children are at even greater risk, rates of CPS reporting and detection are plummeting. Here in Wisconsin, in the four weeks following the stay-at-home order which went into effect on March 15, there was a 48% decrease in CPS reports in Wisconsin as compared to the same time period last year.
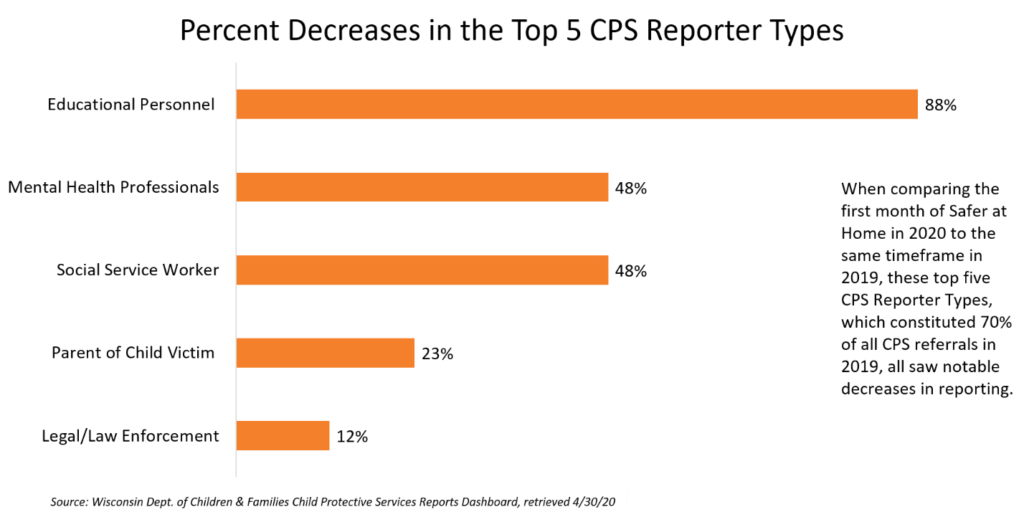
It is unlikely that this trend reflects a true decrease in abuse and neglect, but rather the social isolation of children from mandated reporters. Roughly two-thirds of CPS reports come from professionals such as teachers and doctors. Yet, as shown in the figure below, their reporting has dropped significantly, because they cannot report what they cannot see or hear.
The Child Protection System
If children do come to the attention of CPS, they are now entering a system that is experiencing a period of instability due to COVID-19. Core functions of the child welfare system have been compromised because of the crisis, not unlike other systems. For example, child welfare agencies have been forced to move away from in-person visits where parent-child interactions can be observed directly. Access to substance use and mental health treatment has been reduced significantly. Staffing shortages and court closures have caused delays in removals and permanency decisions.
Disruptions in regular activities are producing a growing backlog of demand for services inside and outside the system. As stay-at-home policies are relaxed, CPS workers who already carry substantial workloads may face even greater job strain, which could lead to high rates of staff turnover. Worse still, assuming the current rate of abuse and neglect reporting is artificially low, the CPS system should be prepared for the coming spike in referrals, substantiations, and out-of-home placements. These impacts are most likely to affect low-income communities of color that are already overrepresented in the CPS system. Disparities in CPS involvement seen before COVID-19 may be compounded by the disproportionate health and economic burdens that these groups are bearing during the crisis. People around the CPS system have been quickly finding new ways of adapting to the social distancing restrictions and accompanying financial hardships, developing clear guiding principles for planning, as the current economic and public health crisis threatens to take a heavy toll on our nation’s most vulnerable population of children and youth.
The Time for Prevention
With state and local governments facing acute budget shortfalls, and with the loss of revenue due to massive increases in unemployment, the need to focus on the most urgent child welfare challenges is clear. And it may seem untimely to increase funding for prevention services that may not pay off immediately, even if these investments tend to yield greater returns in the long run. Although Wisconsin allocates less than 5% of total child welfare funding to prevention services, it may be difficult to justify increased support for anything other than essential responses to known child safety concerns.
On the other hand, the COVID-19 crisis has exposed frailties in the child welfare system, and it is this kind of shock that could force us to reexamine our priorities and rebuild a system that simultaneously ensures the safety, stability, and well-being of children and families. Before this crisis emerged, there were positive signs of movement in this direction with the passage of the Families First Prevention Services Act (FFPSA). Signed into law in 2018, the FFPSA reforms federal child welfare financing by increasing the scope of evidence-based prevention and intervention services that are reimbursable. This includes proven approaches that already have strong roots in Wisconsin such as parent-child interaction therapy, trauma-focused cognitive behavioral therapy (TF-CBT), and evidence-based home visiting.
We believe that our recovery efforts can include plans for increased public investment in prevention services that support families without compromising the vital mission of protecting vulnerable children. It can be difficult to prepare for the future during times of uncertainty and crisis, but bold visions can set in motion lasting change. Let us rebuild our neglected service systems to provide universal, equitable, and accessible services for families and communities.
Learn More
What COVID-19 Means for America’s Child Welfare System – Brookings
Looking Ahead: The Nation’s Child Welfare Systems after Coronavirus – The Chronicle of Social Change
COVID-19 Resources – Children’s Bureau
Legislative Recommendations – Child Welfare League of America
Mental Health in Times of COVID-19
While the health and economic consequences of the coronavirus pandemic are readily apparent, its effects on our collective mental health are less recognizable. Many pundits speculate that a mental health crisis is brewing because stressors accompanying the pandemic reflect the very conditions that impair mental health. These include:
- Environmental catastrophe and community disruption
- Economic insecurity and unemployment
- Social isolation and stressed social relationships
Since the emergence of the COVID-19 crisis in the U.S., Americans everywhere have been exposed to the above-mentioned determinants of poor mental health. Add to the list sickness or death of a loved one during quarantine, and it’s fair to suspect that the population is enduring a collective challenge to its mental well-being unlike any in recent memory. Moreover, families of low-income or racial/ethnic minority status are disproportionately affected by these risk factors, suggesting that they are experiencing extraordinary pressures on their mental health.

Recently released information offers preliminary support for the conclusion that our collective mental health is wavering. For example, calls to crisis hotlines nationwide have jumped nearly nine-fold since the beginning of the crisis, and surveys indicate that nearly half of Americans report negative mental health effects of the pandemic. Low income respondents report mental health effects at even higher rates.
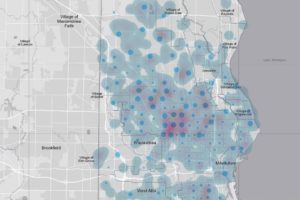
There is also reason to believe that the stress associated with the pandemic is overwhelming Milwaukee area residents. Calls to the local 211 crisis helpline have jumped significantly since the coronavirus outbreak in March. Additionally, Children’s Wisconsin is reporting an unexpected rise in psychiatric emergency visits.

Relative to other Milwaukee enclaves, Milwaukee’s communities of color may be experiencing even higher prevalence of mental health problems. African Americans account for around 65% of the deaths in Milwaukee County due to complications from COVID-19, but only make up about 40% of County residents. Latinx Milwaukee neighborhoods have also seen a recent surge of coronavirus infections and deaths. Both Milwaukee communities, Black and Latinx, tend toward lower income and experience disparities in social and health outcomes. Unfortunately, it is not surprising that families in these communities are bearing a heavy disease burden; nonetheless, it’s important to recognize that the persistent threat to their collective physical health coupled with the secondary consequences of the pandemic could be undermining their mental health in unprecedented ways.
Worse yet, while mental health needs are likely rising exponentially, access to services is probably dropping precipitously. Families of color in Milwaukee with low annual household incomes already face multiple barriers to quality mental health care, including inadequate health insurance coverage, limited availability of care providers, and stigma associated with treatment. Add to these obstacles the current environment of social distancing, and it would seem that many families will go without needed mental health treatment. This is a big problem that warrants a multi-pronged response.
Two solutions rise to the top of our priority list. We at the Institute for Child and Family Well-Being have a history of exploring and providing telemental health services to families with low annual incomes enrolled in public services such as child welfare. For these families, the Institute plans to expand telemental health provision of evidence-based, trauma-informed treatments. These include Parent-Child Interaction Therapy and Trauma-Focused Cognitive Behavioral Therapy. Using a well-established tracking and supervision system, we will ensure high quality service delivery. Recent changes in patient privacy protections allowing for more liberal use of telehealth treatment during the pandemic, along with greater access to online technologies among lower income families, should help facilitate this plan.
In addition, the Institute will continue to train local providers in the delivery of these treatment services. Graduate students from the University of Wisconsin-Milwaukee join the Institute as clinical interns and complete a one-year training apprenticeship. A federally-funded grant also enables the Institute to train over 100 area professionals in the aforementioned intervention types. Institute trainings will now include support for telemental health, and Institute trainers will recruit students and clinicians committed to serving Milwaukee families eligible for public services. Mental health care for these families, who typically experience disorders such as depression and anxiety at astronomically high rates, is critical now more than ever.
Research and Evaluation
The Institute accelerates the process of translating knowledge into direct practices, programs and policies that promote health and well-being, and provides analytic, data management and grant-writing support.
Evaluating Systems Change: An Inquiry Framework
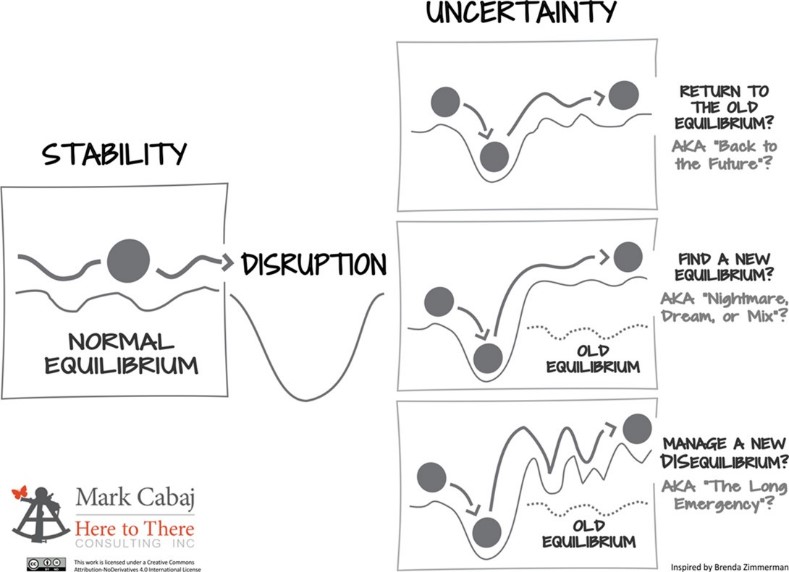
The Institute for Child and Family Well-Being was proud to host the webinar “Evaluating Systems Change: An Inquiry Framework” with evaluation innovator Mark Cabaj, President of Here 2 There Consulting. In this webinar, Mark and ICFW Co-Director Gabe McGaughey discussed why we need to focus on systems change, measuring system change results in uncertain times, with a focus on how strategic learning can be used in times of uncertainty using Developmental Evaluation. Developmental Evaluation combines the rigor of evaluation, being evidence-based and objective, with the creative and adaptive thinking needed to support innovative and rapidly evolving strategies that are typical in systems change efforts. Will the system environment be returning to ‘normal’ quickly, or are we entering a phase of extended uncertainty? What are some questions to ask in applying an Inquiry Framework lens to the child protection system in this uncertain era of COVID-19?
What are the boundaries of the ‘CPS System’ and why change it?
The first step of an Inquiry framework, or any system change effort, is to define the boundaries of the systems and the actors within it. Almost 21% of all CPS reports in Wisconsin made in 2019 came from education personnel. Another 19% from legal/law enforcement. How might those actors be included in improving a system challenged by COVID-19? Minority communities are both disproportionately represented in foster care and the negative health and economic impacts of COVID-19. Can families with lived/living experience in the CPS system contribute to new solutions?
What do system change results look like?
The Inquiry framework outlined three types of results that could be applied to child protection systems.
- Systems Change: The extent to which efforts change the systems’ underlying complex issues, including changes in drivers of system behavior, such as policy, mental models, or resource flows.
- Mission Outcomes: The extent to which efforts help make lives better for individuals, targeted geography/groups, or populations.
- Strategic Learning: The extent of efforts to uncover insights about what we are doing, how we are thinking, and how we are being that are key to future progress.
Recognizing that we’re operating in a crisis context, with rapid change and an uncertain future, focusing on Strategic Learning may elevate insights central not only to the current COVID crisis, but emergent solutions that could be carried forward into future practice.
Strategic Learning
Strategic Learning is the intentional practice of collecting information, reflecting on it, and sharing the findings to improve the performance of an organization or system and inform its direction. With the rapid development of solutions in response to the crisis across the industry, how might we surface solutions that were developed? Adding structure to this process can cut through noise and add efficiency to adapting to an uncertain, and potentially chaotic, environment.
Systems often look for the right tool at the right time to collect information to move forward. Using the correct clinical assessment tool can help separate out trauma from mental health symptoms, leading to more efficient and effective treatment of individuals. Systems are no different. The COVID crisis has already challenged CPS and other systems that support families in unforeseen ways, which are likely to continue for the foreseeable future. Using the right tools at the right time that can evaluate adaptive efforts, can support improving systems and their ongoing efforts to meet the complex needs of families.
Learn More
More resources from Mark Cabaj
FSG resources on Strategic Learning and Evaluation
Program Design & Implementation
The Institute develops, implements and disseminates validated prevention and intervention strategies that are accessible in real-world settings.
Clinical Training Adaptations: PCIT-Toddlers
By Kate Bennett

Reflecting upon the many impacts of the COVID-19 pandemic over the previous few weeks, it’s likely true that each of us have witnessed extraordinary examples of both strengths and challenges affecting individuals, families, and communities. ICFW relies on strategic learning as a way of framing such challenges, with a goal of informing quick adjustments in what we do in our day-to-day work. With shelter-at-home orders in place, the mental and behavioral health needs of families with young children in our community is elevated now more than ever before. For this reason, rapid adaptation has been a standout theme for our team over the last seven weeks.
As we all were pressed to quickly adjust our work and home lives in March, our agency was faced with a question as to whether Children’s Wisconsin would be able to move forward with a previously scheduled in-person Parent-Child Interaction Therapy with Toddlers (PCIT-T) training for mental and behavioral health clinicians. PCIT-T is an adaptation of Parent-Child Interaction Therapy (PCIT) that focuses on meeting developmental needs of children ages 12-24 months through live coaching of a parent or caregiver.1 The 2-day PCIT-T workshop was to take place on March 19-20, just within a week of our team’s transition to home-based work.
Expanding access to early childhood mental health services is a top priority at Children’s, so it was imperative to make sure this workshop could still be offered to clinical staff. ICFW was able to collaborate closely with our PCIT-T trainer, Emma Girard, Psy.D., to determine how we might be able to move forward with this training opportunity knowing that our clinics were physically closing, and an in-person workshop was no longer an option. With a focus on how to continue the dissemination of evidence-based prevention and clinical practices to the many families in need in Milwaukee and beyond, Dr. Girard graciously agreed to adapt PCIT-T training to a web-based format for the very first time with our ICFW and Children’s clinicians as her test group. She worked with our team to create an engaging transition to two 8-hour days of training over Zoom Video Conferencing2, providing well-being baskets filled with PCIT-T themed treats to each clinician participant. ICFW assisted Dr. Girard in ensuring delivery of all training materials to our Milwaukee-based clinicians, and we teamed to provide supplemental training materials to participants through the Basecamp project management and team communication tool.3

From California, Dr. Girard logged onto Zoom shortly after 6am Pacific Standard Time in order to meet clinician need for virtual connection for two full days. Each of the 13 participants joined PCIT-T training from separate locations and remain engaged while Dr. Girard incorporated games, activities, and props into the 16 hours of skills-learning and practice. Reflecting on the experience of training from afar, Dr. Girard indicated that although the process of large-scale distance presentations requires a great deal of energy and planning, she was grateful to be able to offer the physically-distanced workshop to our group of clinicians and was pleased the outcome will provide nurturing and sensitive caregiving practices by brining PCIT-T into the homes of families. We are grateful for her dedication, flexibility, and the thoughtful learning atmosphere she provided.

Additionally, we are nothing short of impressed that Dr. Girard was able to deliver this same training over Zoom for a second PCIT-T clinical cohort grounded in New York the following week. Taking her lead from this web-based experience, Children’s Wisconsin and other Milwaukee-based agencies are now rolling out extensive telehealth services that allow clinicians to engage with families remotely. Utilizing the same HIPAA-compliant technology, clinicians are providing PCIT-T and other evidence-based interventions through video visits with young children and their caregivers. This platform allows continued connections through a child’s MyChart account and is simply accessed by a parent from a mobile device.5 Our mental and behavioral health teams at Children’s and ICFW look forward to continuing the expansion of treatment for kids and families in their natural home environment.
Learn More
Parent-Child Interaction Therapy with Toddlers (PCIT-T)
Children’s Wisconsin Telehealth: Video Visits
References
1 Girard, E.I., Wallace, N.M, Kohlhoff, J.R., Morgan, S.S.J., and McNeil, C.B. (2018). Parent-Child Interaction Therapy with Toddlers: Improving Attachment and Emotion Regulation. New York: Springer.
2 Zoom Video Conferencing, Web Conferencing, Webinars, Screen Sharing. (2020). Retrieved April 27, 2020, from https://www.zoom.us/meeting
3 Basecamp Project Management and Team Communication Software. (2020). Retrieved April 27, 2020, from https://basecamp.com/
4 Girard, E. I., Wallace, N. M., Kohlkoff, J. R., Morgan, S. S. J., & McNeil, C. B. (2020). Parent-Child Interaction Therapy with Toddlers (PCIT-T): Improving Attachment and Emotion Regulation. Retrieved April 27, 2020, from http://www.pcit-toddlers.org
5 Children’s Wisconsin: MyChart. (2020). Retrieved April 27, 2020, from https://chw.org/patients-and-families/mychart
Building Brains with CARE

Building Brains with CARE is an experiential knowledge and skill-building platform. ICFW clinicians have been presenting Brain Architecture: ACE’s, Trauma and Resilience for several years which include the Brain Architecture Game. The Brain Architecture Game is a kinesthetic game experience that helps participants understand the powerful role experiences play in early childhood brain development, those that contribute to strong brain function and those that threaten or hinder it. The entire presentation provided foundational knowledge of Adverse Childhood Experiences (ACE’s), the associated physical and neurological changes to the brain and bolstering resilience in youth, but also was useful those with prior exposure to these concepts. Many of past participants had some base knowledge (i.e. had heard of ACE’s and Trauma-Informed Care) and found the experiential nature of the presentation provided more concrete and eye-opening understanding of their prior knowledge. However, the presentation often left the audience, and presenter, wanting more by way of strategies and tools to help children struggling with effects of toxic stress.
This is where Child-Adult Relationship Enhancement (CARE) comes in. Clinicians were formally trained in the Parent-Child Interaction Therapy adaption by master trainer Christina Warner-Metzger, PhD. After a lot of hard work by Lead Clinician Kate Bennett, and with the support of the iCARE Collaborative, Building Brains with CARE was born and became one of only two applications of CARE outside its initial designed scope granted by the iCARE Collaborative in the nation. Building Brains with CARE is a combination of in-person concept introductions and virtual learning and practice. This format is used to celebrate learning and gaining mastery in concepts and new skills.
After an initial in-person session, each cohort gains access to a Building Brains with CARE Community of Practice. ICFW clinicians and participants utilize Zoom Web Conferencing to virtually engage with each other to revisit and complement in-person information. Additional resources can be provided by ICFW clinician participants, everyone practices skills and shares how they’ve tested the implementation of knowledge through the Plan-Do-Study-Act cycle. The Community of Practice topics are flexible as different avenues of discussion are based on participants’ interests, findings and sharing. Basecamp, which is an easily accessible project management platform, is also used to share resources, enable interaction and act as a living archive of discussions and learning objectives.

During the in-person and virtual Community of Practice, participants practice identifying situations that may indicate common trauma reactions and skills they can use within their relationships that support resilience and healthy communication. They have the opportunity for family consultations, skill-building and access to bibliographic resources. Participants learn which evidence-based interventions may be useful to families who are experiencing significant impairment in functioning due to trauma exposure.
While content is traditionally introduced over the course of one day with participants then gaining access to virtual resources including live Community of Practice sessions, there have been a few adaptions made to accommodate audience. Prior to COVID-19 changed so many things, UWM Children’s Learning Center approached ICFW to inquire about schedule flexibility in order to be worked into their pre-established professional development time. ICFW set off on adapting the Building Brains with CARE in-person format from a one-day session to five 2-hour sessions. After social distancing expectations were put in place, ICFW clinicians worked to adapt session three from in-person to Zoom-based in order to carry on with our collaboration with UWM Children’s Learning Center. Building Brains with CARE will soon be available through the Professional Development System at the UWM Partnership. If you’d like to learn more about how to get involved, please contact Luke Waldo at lwaldo@chw.org.
Learn More:
Building Brains with CARE
Recent and Upcoming Events
The Institute provides training, consultation and technical assistance to help human service agencies implement and replicate best practices. If you are interested in training or technical assistance, please complete our speaker request form.
ICFW Webinars:
April 8th
Evaluating Systems Change: An Inquiry Framework For Uncertain Times
April 16th
Authentic Community Engagement: Made in Milwaukee
May 4th
Making the Unspeakable Speakable: Making a Case for Trauma Screening and Assessment
May 20th
Parent Child Interaction Therapy in Child Welfare
June 17th
Trauma screening, brief intervention and referral to treatment (T-SBIRT): Introduction to a promising, brief protocol for social service and healthcare settings
Trainings:
May 11-13 (Postponed)
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) Learning Collaborative – South Milwaukee
May 14-15 (Postponed)
Sustaining Advanced Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) Practice Session – Madison